Table of Contents
- Introduction
- Marketing “Upstream” of Behavior Change
- How Effectively Do Communications Shape the Behavior Cascade?
- Take-Home Points
Introduction
We recently posted on the innate challenges of using persuasive communication to change healthcare-related behaviors, and we shared evidence that, in fact, healthcare is a tougher setting for driving behavior change. In our next series of posts we want to paint a more optimistic picture by highlighting key findings from science that point to things we can do to improve communication content in ads and other vehicles for communications to make them more effective. In this short summary, we show how persuasive communication works to influence different elements of the “behavior cascade” – a term we use to mean the set of upstream conditions that need to exist for behavior change to occur.
Marketing “Upstream” of Behavior Change
Marketers in life sciences often have to think like sophisticated psychologists when they are deciding what they want to achieve with communications to customers. They recognize that changing behavior through persuasive communication is often a multi-step process – where a variety of dynamics must fall into place “upstream” before behavior change can occur. Additionally, they know that customers and markets often have to go on a bit of a mental and emotional journey before they are ready to change. In many cases, marketers have to start by meeting customers where they are today. So while we might glibly say that all customer communication is designed, ultimately, to drive customer behavior (and thus sales), the reality is that marketing communications have diverse goals. Academics have devised various healthcare-specific models to characterize what we ordinarily think of as the “behavior cascade” – a series of internal and external conditions that need to be met in order for behavior change to occur. A popular example in healthcare and public health communications is the Stages of Change model, which conceptualizes health behavior changes as a time-extended commitment process. Rather than concern ourselves with these frameworks, we want to look at the elements that are common to most of them, because these elements are the primary upstream targets for marketing.
- Shaping Beliefs:
- Some persuasive communications are designed to intervene at the top of the behavior change cascade. One important way to do this is by updating beliefs – the basic understanding we carry with us about how things work. Beliefs could include:
- Understanding about disease prevalence or the lived experience of a particular condition
- Understanding about the action and logic of a treatment’s activity in the body
- Increasing empathetic comprehension of what patients’ and caregivers’ subjective experiences are like
- Illuminating a problem that can be solved through the use of a treatment
- In fact, it can be argued that, because of healthcare’s cultural emphasis on science (i.e., using evidence to update our understanding of the world), almost all communications have some degree of focus on belief-shaping.
- Some persuasive communications are designed to intervene at the top of the behavior change cascade. One important way to do this is by updating beliefs – the basic understanding we carry with us about how things work. Beliefs could include:
- Shaping Attitudes:
- Communications are commonly designed to alter the type, intensity, or valence of an emotional association with a product or a company. This kind of communication is focused on attitude-shaping. While attitudes by themselves are usually (but not always) weak predictors of behavior, when examined in the context of other factors, they can become big levers. Communications designed to shape affective response are very common in healthcare.
- Social Norms:
- Even in a science-centric arena like medicine, humans are still human. And social norms play a huge role in driving behavior by establishing what is regarded as ordinary and socially or culturally acceptable. Many people are reluctant to act in opposition to norms, even if they hold beliefs or attitudes that suggest they ought to. But when beliefs and norms align, behavior intention tends to be strong. Communications can be used to either shape norms by altering beliefs en masse, or to alter the perception of what the social norm is in the mind of the receiver.
- Perceived Control:
- Psychologists use a range of terms to refer to the idea that people see themselves as having different degrees of agency in their lives and particularly in health-related decisions. A key aspect of this is the extent to which the communication target believes he/she is able to influence the behavior or outcome in question. Recognizing this, marketers often create communications designed to create a recognition of agency. For example, communications might be devised to change how customers perceive real or imagined behavioral barriers.
- Intent:
- Most models of behavior change reflect the importance of intent – the state where the behavior in question is “on the docket” in the mind of the customer. Though occasionally we make the mistake of assuming that intention by itself is adequate to predict behavior (see, e.g., discussion by Rhodes & Dickau, 2012 or Hagger et al, 2016), the evidence is clear that intention is just one necessary pre-condition to deliberate behavior change in healthcare (and most settings).
All of these examples of marketing endpoints underscore the point that there are a range of ways that you can help to prepare customers for new behaviors without driving directly at behavior. This is a bit like setting up a garden, where creating the right soil and nutrient conditions, access to sunlight and protection from predators are all precursors to growing vegetables or flowers.
How Effectively Does Communication Shape the Behavior Cascade?
Clearly, all of these endpoints are a bit different from each other, and so a marketer might reasonably wonder whether communications can shape these diverse types of outcomes with any degree of consistency. We have seen in prior summaries that behavior change is actually fairly reliable as an outcome. But what do we know about shaping attitudes or norms? After all, we hear in some settings that attitudes are particularly difficult to change. And we are also reminded that updating beliefs can actually be very challenging due to backfire effects and misinformation effects (Chan et al, 2017). With the burgeoning literature on message effectiveness, we are in a position to unpack this question fairly precisely.
Example #1: Effects of Simple Written Communications on Various Marketing Endpoints
An early meta-analysis, published in 2003 and authored by Dolores Albarracin and colleagues, thoroughly examined the impact of persuasive communication on condom use among at-risk populations for HIV transmission. The authors tackle our main question directly by examining the effects of simple, one-shot persuasive communications relating to condom use and its relationship to the transmission of HIV. The meta-analysis examined the range of communication effects across a range of variables related to the behavior change cascade, including attitudes toward condoms, perceptions of personal risk, knowledge about condoms and HIV transmission, intention to use condoms and actual condom use. The published findings include both fixed and random-effects results, which, as is usually the case in meta-analysis of communication research, were highly similar, and I have elected to show the random-effects outputs here for simplicity. I converted their report d values to rES to make the results comparable to other meta-analyses that we will discuss. As always, we convert the effect size into more practical terms using our “bodies moved” indices where we conceptualize the communication effect in terms of the proportion of people exhibiting the outcome relative to arbitrary baselines of 10% and 30%.
Table 1: Effects of Simple Written Communications on Different Marketing Endpoints Related to Condom Use
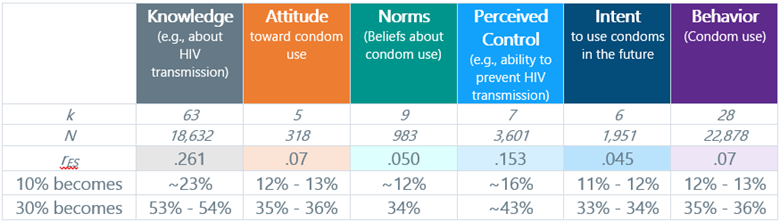
As is always the case with meta-analyses, not every study represented all of the different communication-impact endpoints, which is why the k (number of studies) and N (total humans) values vary.
It is not surprising to see these types of effects because of the subject in question (condom use) is a mediator of two competing, intense and emotional outcomes (health/safety vs. sexual pleasure). We can see that objective endpoints (like knowledge and perceived control) are more malleable to persuasive communications. Secondly, where communications intersect with more complex phenomenon (like feelings or perceptions of social norms), the effects can be more complicated. For some readers, the similarity in effect size between intent and behavior might be surprising because reporting intent to use condoms does not imply any genuine commitment to doing so. However, as we will see, this is a common pattern we see across domains. Generally speaking, people can and will say what they intend to do, and such data ought to be taken as a serious index of what their behavior will be (see comments by Fishbein & Ajzen, 2011). In this case, reluctance to use condoms despite amplification in knowledge and bolstering of perceived control is a genuine signal about just how hard it is to engender this behavior. Also, keep in mind that this analysis was focused on the effects of one-shot written communications. That kind of intervention is pretty minimalistic in comparison to the kinds of promotional ecosystems we can create today, and so we can expect to have larger effects when communications are repeated and supported with alternate media.
Example #2: Effects of Narrative-Based Communications on Various Marketing Endpoints
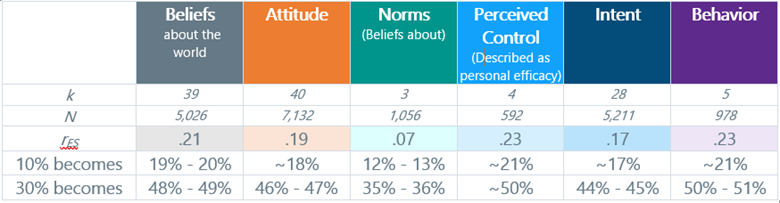
Toward that end, a more recent meta-analysis, published in 2016, looked at the effect of communications that used narratives (i.e., fictional vignettes about characters) to influence elements of the behavior cascade. This synthesis was domain general in that it did not focus exclusively on healthcare. However, we already know from a prior post in this series that healthcare communication effects tend to be smaller, so we can simply make the mental “correction” as we review these findings – simply assume that these effects would be 40% to 50% smaller in healthcare-related communications. Clearly, the narrative-based communications tested in these studies are more potent compared with the strict fact-centric communications used in most of the studies in the Albarracin et al meta-analysis, and this is further amplified by the fact that this analysis included many studies outside of healthcare, where behavior change is normally easier.
Table 2: Effects of Narrative-Based Communications on the Behavior Cascade
Example #3: Effects of Communications on Attitudes, Intention, and Behavior
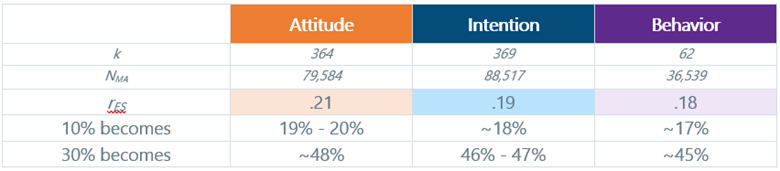
We see similar effect size alignment across some of our major marketing outcomes in a sweeping 2022 meta-analysis that included more than 700 published experiments and more than 200,000 participants. Up to this point, I am unaware of a more comprehensive database from which to draw scientific conclusions about persuasive communication effects. Their summary of communications impact on several behavior cascade endpoints is shown in Table 3 below. The authors of this study were examining a much broader set of topics than what we are discussing in this piece, and the set of endpoints they considered was narrower than the other studies. Still, the sheer size and analytic power of this study underscore an important conclusion: persuasive communications generally produce similarly sized effects on major marketing endpoints. Unfortunately, the authors did not examine any aspects of belief change, impact on perceived norms, or personal control.
Table 3: Impact of Persuasive Communication on Parts of the Behavior Cascade
It is worth noting one other major finding about persuasion effects on beliefs. A meta-analysis on the use of messaging to counteract misinformation (see Chan et al , 2017) confirmed that the message-belief relationship is indeed predictably large. This work demonstrated that after being exposed to misinformation, corrective messages were correlated at rES =.83 with belief change. This enormous effect is mediated by the types of experimental tasks used in the attendant studies, and in my estimation, it is probably somewhat inflated. But the important point is that it does reinforce that belief updating is generally going to be an easier target for marketing efforts, relative to downstream behavior.
Take-Home Points
There are several major conclusions for marketers and insights professionals to draw from this summary, which can be helpful in mapping the kinds of interventions and investment that may be needed to achieve our commercial goals.
- POINT #1:
- Communications can meaningfully influence essentially any dependent variable of interest, but we should expect that some aspects of the behavioral cascade will require more persuasive effort than others.
- POINT #2:
- Belief-updating, which includes refinement of factual understanding as well as perceptions of personal control/agency are ordinarily going to be easier to update. In this sense, marketers may be able to successfully use more population-general and less targeted styles of communications that are not explicitly matched to the underlying motivations of customers to achieve their goal of updating the mental models of customers.
- POINT #3:
- Motivation-related targets, specifically attitudes about the behavior/object and intentions – are more difficult to alter. However, the expected effect sizes will be similar irrespective of the endpoint the marketer is focused on. We will talk about methods to increase the potency of motivation-related endpoints in a separate post.
- POINT #4:
- Communications effects are generally modest even under idealized conditions. However, when we translate the odds-ratios into “percent of bodies moved” metrics (see last two rows in each table), the results remind us that the “juice is worth the squeeze.”
Relevant Topic: We also explore the persuasive power that we can capitalize on by using different communication media and channels. And we see how big the differences are in what we can achieve when we invest in them. See our post titled “How Much Does Media & Channel Selection Matter in Healthcare Communications?“
To learn more, contact us at info@euplexus.com.
About euPlexus
We are a team of life science insights veterans dedicated to amplifying life science marketing through evidence-based tools. One of our core values is to bring integrated, up-to-date perspectives on marketing-relevant science to our clients and the broader industry.
References
Albarracín, D., McNatt, P. S., Klein, C. T., Ho, R. M., Mitchell, A. L., & Kumkale, G. T. (2003). Persuasive communications to change actions: an analysis of behavioral and cognitive impact in HIV prevention. Health psychology, 22(2), 166.
Braddock, K., & Dillard, J. P. (2016). Meta-analytic evidence for the persuasive effect of narratives on beliefs, attitudes, intentions, and behaviors. Communication monographs, 83(4), 446-467.
Chan, M. S., Jones, C. R., Hall Jamieson, K., & Albarracín, D. (2017). Debunking: A Meta-Analysis of the Psychological Efficacy of Messages Countering Misinformation. Psychological Science, 28(11), 1531-1546.
Fishbein, M., & Ajzen, I. (2011). Predicting and changing behavior: The reasoned action approach. Taylor & Francis.
Hagger, M. S., Chan, D. K., Protogerou, C., & Chatzisarantis, N. L. (2016). Using meta-analytic path analysis to test theoretical predictions in health behavior: An illustration based on meta-analyses of the theory of planned behavior. Preventive medicine, 89, 154-161.
Joyal-Desmarais, K., Scharmer, A. K., Madzelan, M. K., See, J. V., Rothman, A. J., & Snyder, M. (2022). Appealing to motivation to change attitudes, intentions, and behavior: A systematic review and meta-analysis of 702 experimental tests of the effects of motivational message matching on persuasion. Psychological Bulletin, 148(7-8), 465.
Marshall S J, Biddle S J. The transtheoretical model of behavior change: a meta-analysis of applications to physical activity and exercise. Annals of Behavioral Medicine 2001; 23(4): 229-246.
Rhodes, R. E., & Dickau, L. (2012). Experimental evidence for the intention–behavior relationship in the physical activity domain: A meta-analysis. Health Psychology, 31(6), 724.